Melanoma is cancer of the melanocytes, cells that are derived from the neural crest and produce the pigment melanin.1 Most melanomas develop in the skin, but they can also develop from other sites where neural crest cells migrate, such as the uveal tract, gastrointestinal tract, and brain. The content on this website focuses on cutaneous melanoma only.
Pathophysiology
Most melanomas may arise near a precursor lesion or in healthy skin (referred to as “de novo” skin cancer).2 Examples of melanoma precursor lesions include common acquired nevi, dysplastic nevi, and congenital nevi.3
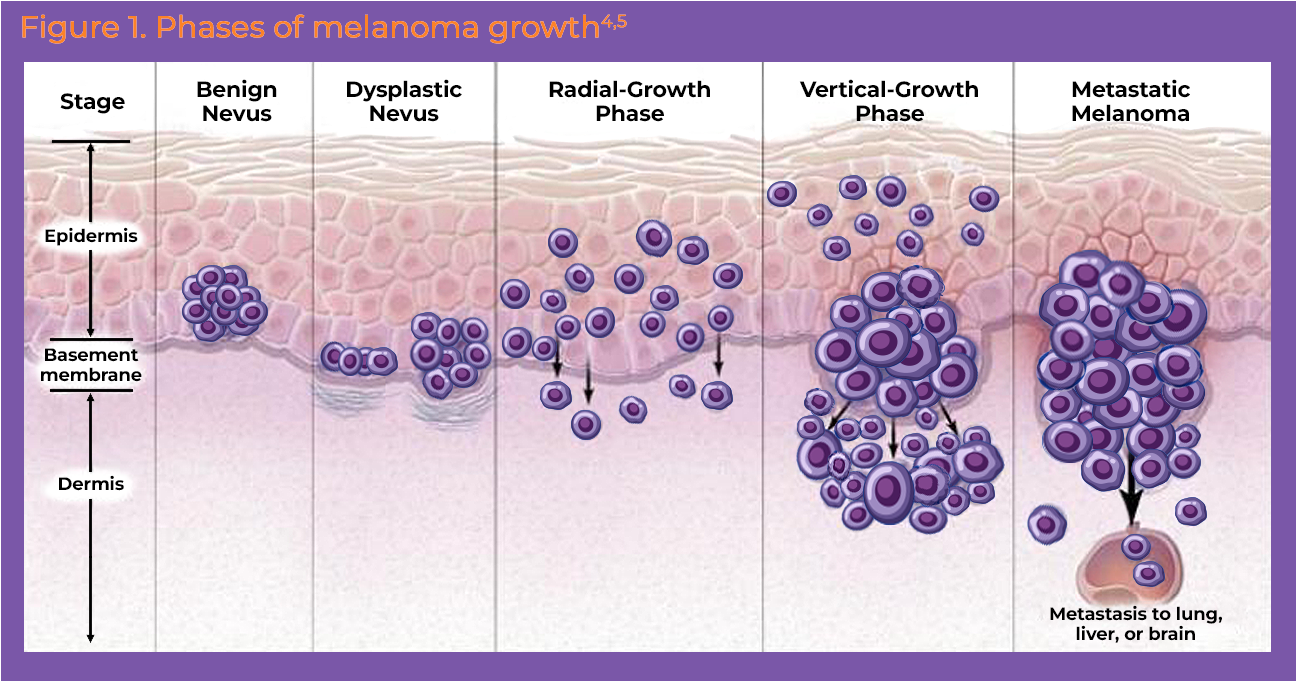
Melanomas grow in 4 stages (Figure 1):
Radial phase: cancerous cells confined to the epidermis grow radially; may last months to years
Vertical phase: melanoma becomes invasive as it penetrates below the epidermis
Tumor thickness: melanoma deepens and thickens
Metastatic: melanoma invades subdermal vessels (ie, lymphatic, blood) and seeds into the circulation4,5
Melanoma Subtypes
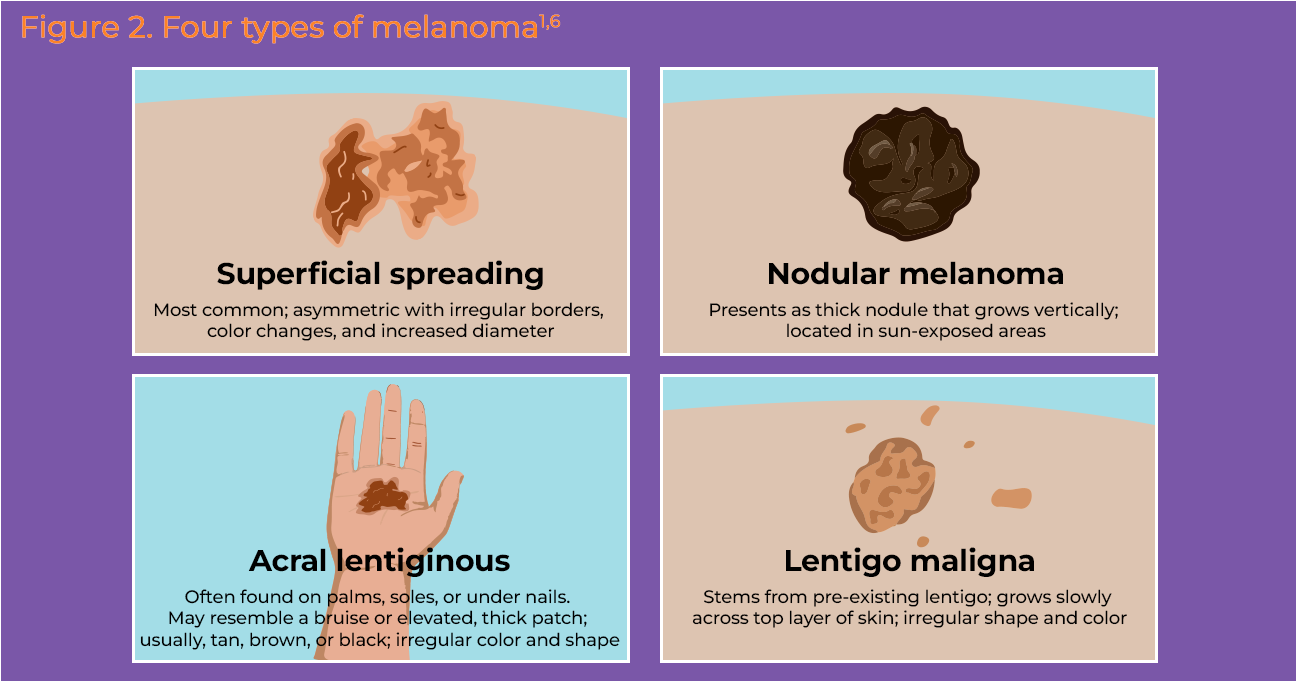
Broadly, the four most common types of melanomas are: superficial spreading melanoma, lentigo maligna melanoma, nodular melanoma, and acral lentiginous melanoma (Figure 2).6-8 Superficial spreading melanoma accounts for about 70% of melanomas, followed by nodular melanoma that accounts for 15% of melanomas.7 Lentigo maligna is seen in older patients and is commonly seen in areas exposed often to sunlight, and accounts for about 5% to 10% of melanomas. Acral lentiginous melanomas make up about 8% of melanomas and typically develop in darker skinned people, sometimes appearing on the palms, soles, and under the nail bed. Subtypes have been found to differ in their gene mutation profile (Table 1). 8
Melanomas can also be classified into 4 major genomic subtypes based on certain genetic alterations and evolutionary tracks.9 These include:
BRAF mutations seen in 50% of melanomas
NRAS mutations seen in 20% of melanomas
NF-1 mutations seen in 10%-15% of melanomas
Triple wild-type seen in 15% of melanomas.9
Stages of Melanoma
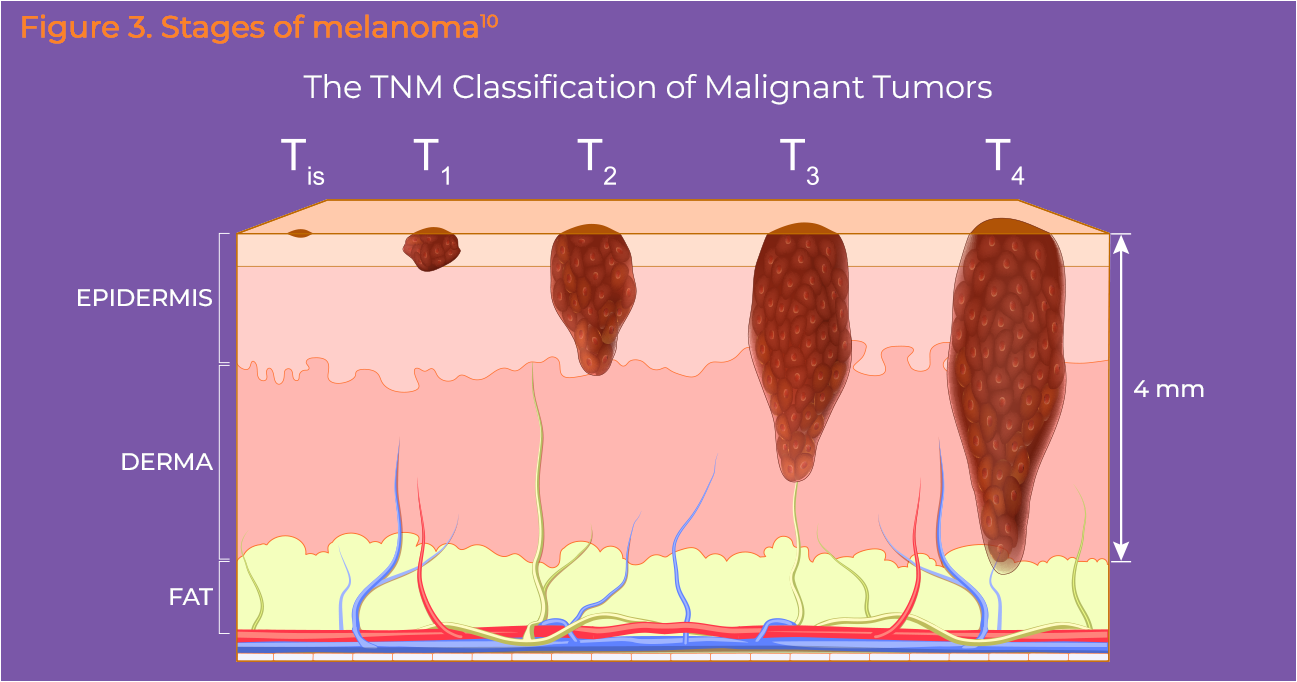
Melanoma staging is usually determined by the American Joint Committee on Cancer (AJCC) TNM (Figure 3).10 T stands for tumor and is used to indicate the thickness of the melanoma (Breslow measurement) and the ulceration or breakdown of the skin over the melanoma. Melanomas that are less than 1 mm thick and those that are not ulcerated have a very small chance of spreading. N stands for lymph nodes, and is used to indicate spread of the disease to nearby lymph nodes. M stands for metastasis and is indicative of whether the cancer has spread to distant skin, lymph nodes, and/or distant organs.10 A sentinel lymph node biopsy can be used for staging of melanomas and further information can be found in the Symptoms and Diagnosis section.11 The 5-year survival rate of patients with Stage IV melanoma is only 5% compared with 100% for patients with Stage 0 melanoma.12
Statistics
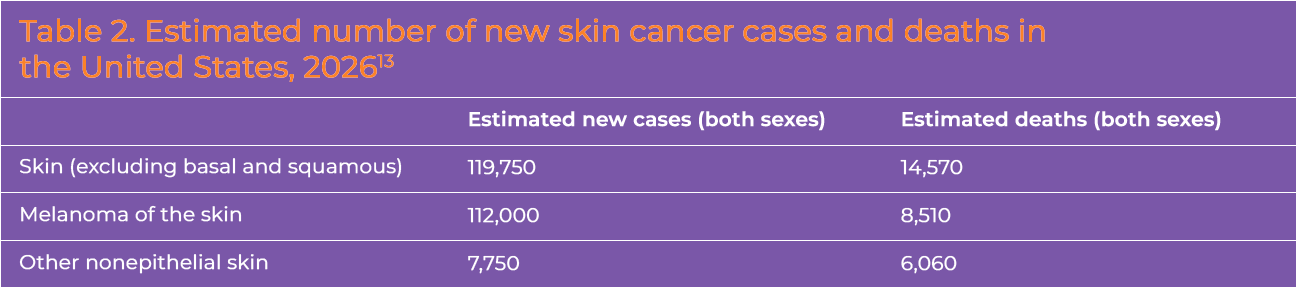
Melanoma is the fifth most common cancer among men and women in the United States (Table 2).13 In 2026, the United States is expected to have about 65,400 men and 46,600 women diagnosed with melanoma.12 The average age of diagnosis is 66 years.10 While the incidence of melanoma was on a sharp rise for decades, rates of invasive melanoma have remained stable among individuals younger than 50 years since the early 2000s, and have actually decreased 1% per year in men over the same time frame.13 Unfortunately, incidence rates are increasing in adults aged 50 years and older and in women. Over the last 10 years, mortality from melanoma has decreased by an estimated 2% per year in women and 3% per year in men, largely due to effective advances in therapy for advanced disease. 12
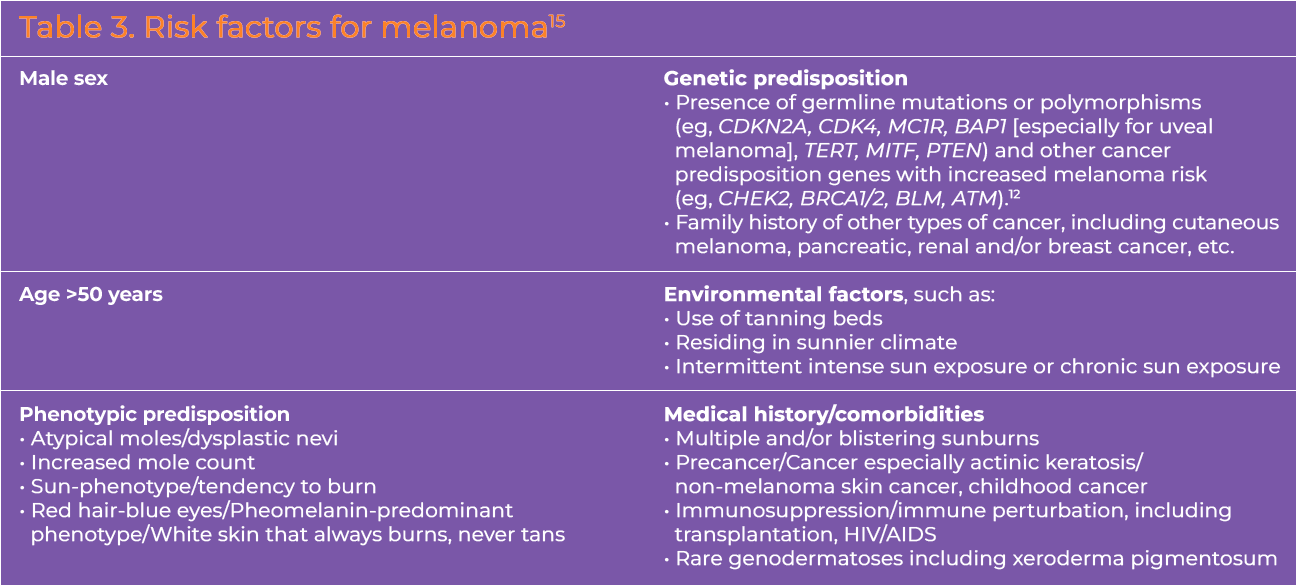
Risk Factors
Outcome of melanoma depends on the stage at which it is detected, and early detection is key to a good prognosis.14 Metastatic or advanced melanoma is one of the most serious forms of skin cancer. Risk factors for melanoma include male sex, age > 50 years, certain phenotypic and genotypic predispositions, personal history and comorbidities, and environmental factors (Table 3).8 It must be noted that melanoma can occur in any ethnic group and also in areas of the body not exposed to sunlight.16
Amaral T, Ottaviano M, Arance A, et al. Cutaneous melanoma: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2025;36:10-30. https://doi.org/10.1016/j.annonc.2024.11.006
Okobi OE, Abreao E, Sams NP, et al. Trends in melanoma incidence, prevalence, stage at diagnosis, and survival: an analysis of the United States Cancer Statistics (USCS) Database. 2024;16:e70697. https://doi.org/10.7759/cureus.70697