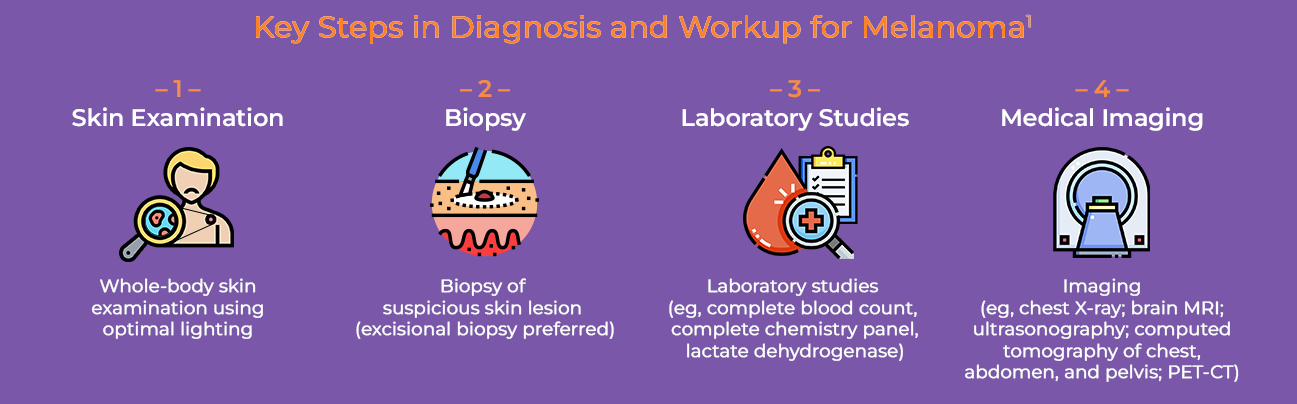
Imaging (eg, chest radiography; brain MRI; ultrasonography; computed tomography of chest, abdomen, and pelvis; PET-CT)
Examination
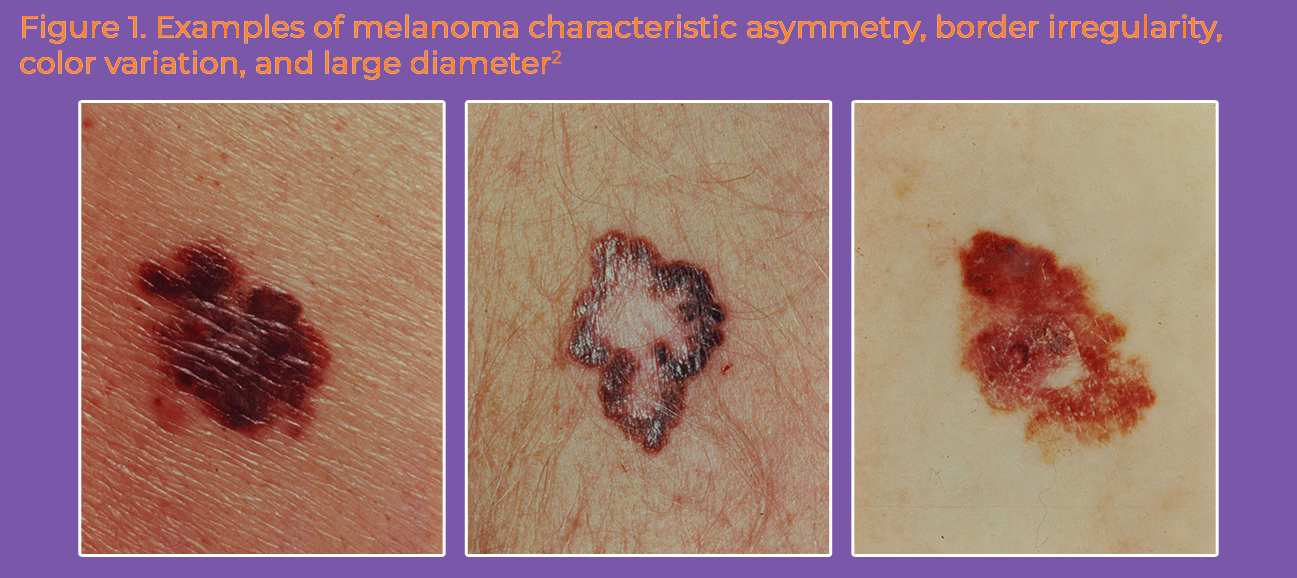
A helpful acronym used to identify suspicious characteristics of a pigmented lesion is ABCDE (Asymmetry of the lesion, Border irregularity, Color variation, Diameter >6 mm, Evolution or change in the lesion), as shown in Figure 1.1,2 Signs and symptoms that may indicate transformation of a precancerous lesion to melanoma include darkening or changing color, itching, increasing size, satellite development, and ulceration or bleeding.1 Patients with metastatic disease will also have signs and symptoms related to the affected organ(s). During diagnosis, all lymph node groups must be evaluated.2
Biopsy and Histopathology
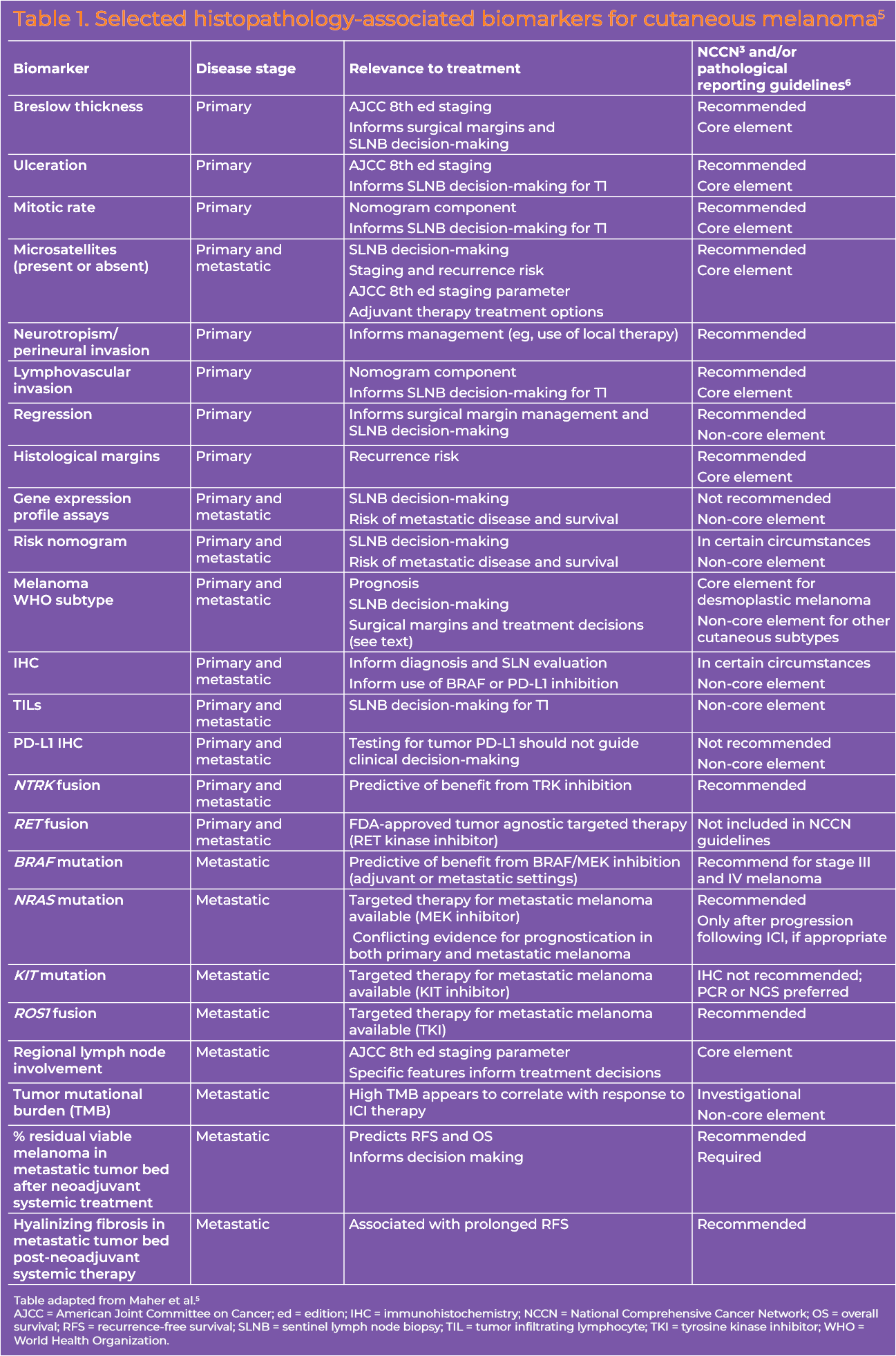
Excisional complete biopsy (1-3 mm margins) is the preferred approach (eg, deep shave removal, punch [for small lesions], elliptical).3 Full-thickness incisional or punch biopsy may be preferred for lesions on the palm/sole, fingers/toes, face, or ear and should be done at the thickest or most atypical part of the lesion.3 Histopathologic evaluation of biopsy specimens is a critical step in melanoma diagnosis and workup. Key features that should be reported are Breslow thickness, ulceration, microsatellites, margin status, dermal mitotic rate, lymphovascular or angiolymphatic invasion, histologic subtype, regression, and neurotropism/perineural invasion (Table 1).3,4
Additional tests to discern malignant from benign lesions that may be considered are: immunohistochemistry (IHC) and molecular testing via comparative genomic hybridization (CGH), fluorescence in situ hybridization (FISH), gene expression profiling (GEP), single-nucleotide polymorphism (SNP) array, and next-generation sequencing (NGS). These tests should be used on a case-by-case basis ancillary to clinical and dermatopathologic examination and should be interpreted within the context of clinical findings.3 Melanomas associated with a greater than 5% risk of having a positive sentinel lymph node can be assessed with a sentinel lymph node biopsy (SLNB) to determine the spread of the cancer to nearby lymph nodes.3