Once your doctors know more about your cancer, such as its stage and where it is in your body, they can start to plan your treatment.1,2 They will try to make the best plan for you based on your melanoma, the risk that it might return after treatment, your health, and what is important to you.2
Ask your doctor about going on a clinical trial for melanoma. Clinical trials are available for all stages of disease.
Types of treatments used for melanoma are: surgery, radiation therapy (RT), and anti-cancer drugs—for example, chemotherapy (chemo), immunotherapy, targeted therapy, or a clinical trial— as show in Table 1.
Your doctor may use just one of these treatments, or you may get more than one. In some cases, your doctor may suggest observation.
If surgery plus other type(s) of treatment are used, your doctor may use words that describe their order.1
Neoadjuvant (before) treatments are given before the main treatment (often, surgery). For some people neoadjuvant treatment may make surgery possible or easier.
Adjuvant (after) treatments are given after the main surgery and help kill any cancer cells left in the body.
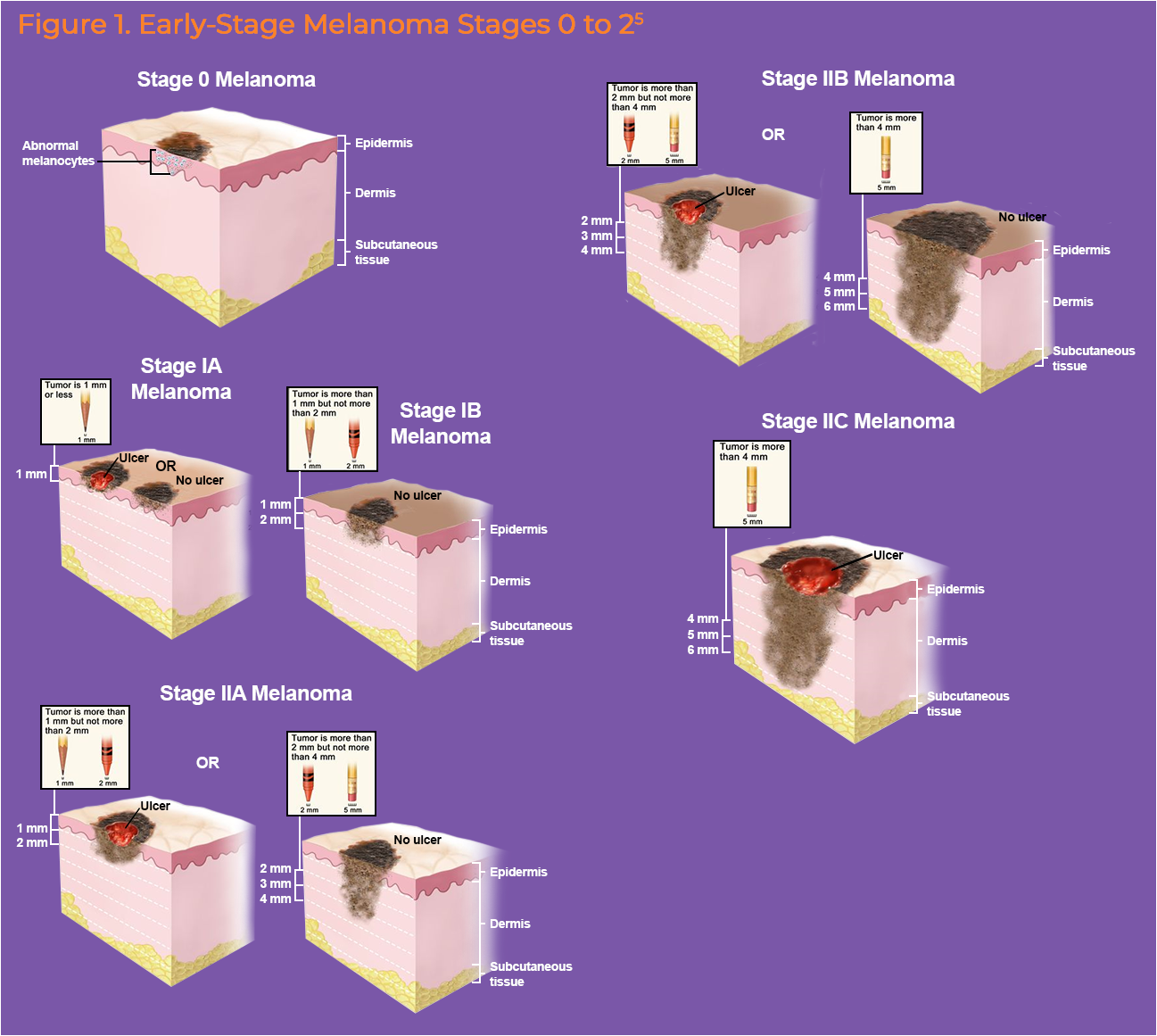
Early-Stage Melanoma: Stages 0 to 2
Melanoma that is stage 0 to 2 is called “early-stage” (Figure 1).1 It responds well to treatment and is curable.1 Surgery is the main treatment used, along with immunotherapy, radiation therapy, and clinical trials.1,2 The surgery used is often a wide excision.1,2
Stage 0 cancer is also called melanoma in situ.1,2 Stage 0 and stage 1A melanomas are often treated with surgery alone.1-3
If your cancer is stage 1b, 2a, or 2c, your doctor may want to do a sentinel lymph node biopsy with the surgery.1 Before surgery, your doctor may order more tests or imaging. If cancer is found in the sentinel lymph node, your cancer will be upstaged to stage 3 (see Regional Melanoma section, below).1
Some patients with stage 1b or stage 2 may get adjuvant therapy after surgery.1,3 Adjuvant therapy may be:1,3
Clinical trial (for stage 2),
Observation,
Immunotherapy for stage 2b or 2c (nivolumab [Opdivo] or pembrolizumab [Keytruda])®, or
In some cases, a patient may get adjuvant RT.
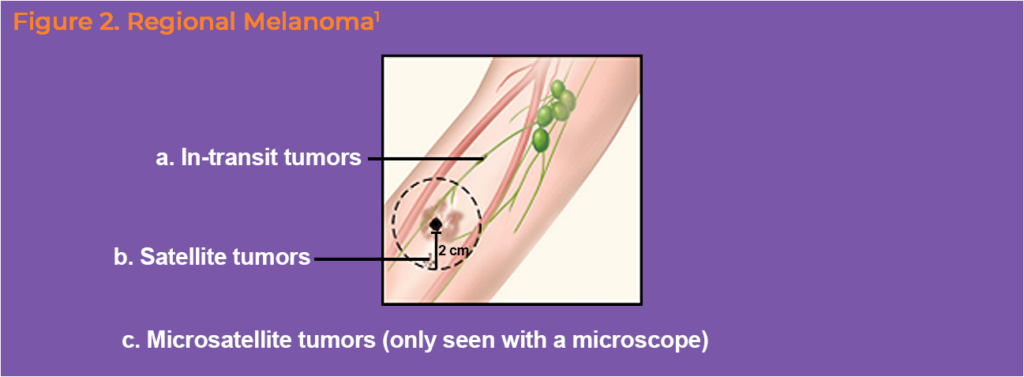
Regional Melanoma: Stage 3
Melanoma that is stage 3 is called “regional” (Figures 2 and 3).1 It has spread to areas close to the primary tumor, but not to parts of the body far away.1,2
Stage 3 tumors may be found:1
In nearby lymph nodes (sometime called node-positive disease)
As tiny skin tumors next to or below the primary tumor (microscopic satellites or microsatellites, Figure 2a)
In the lymph vessels, as deposits that are 2 cm or less from the primary tumor (satellites, Figure 2b). Your doctor will be able to see or feel these when they do a skin exam.
In the lymph vessels, as deposits that are more than 2 cm from the primary tumors, but not yet in the lymph nodes (in-transit tumor, Figure 2c).
Regional melanoma with lymph node involvement
Clinically positive nodes
A clinically positive node means your doctor found an enlarged lymph node before surgery. For example, they may have felt that it was bigger than normal on exam. If that happens, they will take a sample of lymph node cells with a needle (fine-needle aspiration [FNA] biopsy) to look for cancer.
If your cancer is resectable, they may offer you neoadjuvant systemic therapy before surgery (Table 2). The surgery recommended for this is wide excision of the primary tumor with lymph node dissection to remove the lymph nodes that have cancer.
If your clinically node positive melanoma is unresectable, your doctor will offer you systemic therapy, RT, intralesional T-VEC, and/or best supportive care.3
Sentinel lymph node positive melanoma
If your doctor finds cancer in the sentinel lymph node biopsy (SLNB) taken during surgery, they may order more tests. For example, imaging and BRAF V600 mutation testing.1 Imaging may be used to check if there is cancer in other nearby lymph nodes.1 When cancer is found in the SLNB, lymph node dissection (surgery), neoadjuvant or adjuvant immunotherapy, targeted therapy, or RT may be used.1,3 When possible, surgery is the main treatment used.1,3
Resectable regional melanoma
Your surgeon will try to remove all the lymph nodes that have cancer in them. For most resectable 3a tumors, no treatment is used after surgery.1,3 If your melanoma has features that make the risk of coming back high, your doctor may want you to take adjuvant systemic therapy (Table 3).1,3
Unresectable regional melanoma1,3
If the cancer is unresectable, systemic therapy is used (often with immunotherapy or targeted therapy). Your doctor may use RT to help with some symptoms. T-VEC skin injections may be an option for some patients.
Regional melanoma with microsatellites
If your doctor finds microsatellite cancer after biopsy or surgery, your doctor may order imaging, BRAF mutation testing. The main treatment used for melanoma with microsatellites is wide excision surgery with or without SLNB. Other treatments that may be used are adjuvant systemic therapy, clinical trial, or observation. Systemic therapy options include immunotherapy with nivolumab (Opdivo)® or pembrolizumab (Keytruda)® or targeted therapy with dabrafenib and trametinib (Tafinlar/Mekinist, for tumors with a BRAF V600 mutation).
Regional melanoma with satellite or in-transit tumors
Resectable regional melanoma with satellite or in-transit tumors
Treatments used for resectable regional melanoma with satellite or in-transit tumors may be neoadjuvant systemic therapy, surgery (complete excision), T-VEC/intralesional therapy, or systemic therapy without surgery. Neoadjuvant systemic therapies used for this type of cancer are listed in Table 2.
After neoadjuvant systemic therapy, surgery is done to remove the rest of the cancer. If the doctor finds no signs of cancer are left behind after surgery, they say the margins are clear. For clear margins, you may also receive adjuvant systemic treatment after surgery.
If the doctor finds cancer cells left after surgery, your doctor may use T-VEC, RT, or palliative therapy.1,3
Resectable regional melanoma with satellite or in-transit tumors
If your melanoma is unresectable, your doctor may offer an injection of therapy into the lesion with T-VEC (preferred) or interleukin-2 (IL-2), RT, or surgery to help with symptoms.3 T-VEC is the preferred therapy for most patients that can’t undergo surgery.1,3
Melanoma: Metastatic (Stage 4) disease
If you are diagnosed with stage 4 melanoma, your doctor may order more tests to learn out more about the cancer.1,3 This information will help them decide how to treat the melanoma.
Limited Metastatic (Oligometastatic) Melanoma
If your cancer is only found in a few sites in your body (called, “limited metastatic” or “oligometastatic”, your doctors may use surgery, stereotactic RT, or T-VEC injections and/or systemic therapy.1,3 It is important that your doctor consults with your entire cancer care team (for example, surgeons and radiation doctors) to decide the best plan for you.3
Widely Metastatic or Unresectable
If the cancer is widespread or unresectable, you will receive systemic therapy, palliative therapy, and supportive care.1,3 The first systemic therapy you receive for stage 4 melanoma is called the “first-line” of therapy.3 If your cancer grows on first-line therapy, your doctor will switch to a “second-line” of systemic therapy. Immunotherapy is the preferred first-line systemic therapy for stage 4 melanoma (Table 4).